Abstract
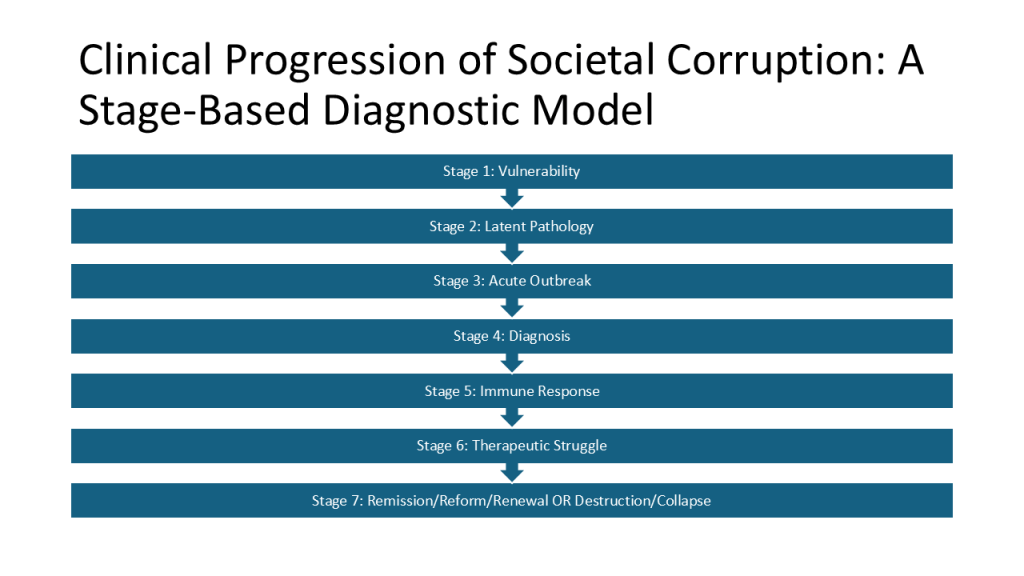
This article proposes a medical diagnostic model for analyzing societal corruption, treating it not as isolated moral failure or ideological conflict but as a disease process with identifiable stages: vulnerability, latent pathology, acute outbreak, diagnosis, immune response, therapeutic struggle, remission, and two potential endpoints of renewal or collapse. The model is applied across fifteen core social institutions: family, education, economy, finance, healthcare, religion, government, law, elections, media, security, science, civil society, culture, and global systems.
While metaphors comparing society to a living organism have appeared throughout philosophical and sociological history, this framework advances a novel synthesis by organizing those metaphors into a structured, stage-based diagnostic system intended for comparative analysis and empirical testing. Rather than prescribing ideology or policy, it offers a clinical lens for identifying patterns of institutional vulnerability, corruption, and recovery.
Intellectual Lineage and Original Contribution
The conceptual foundations of this framework draw from several longstanding traditions in political philosophy, sociology, and public health.
Classical political philosophy, particularly Plato’s notion of the body politic, framed society as an organism whose parts must function in harmony for collective health. Émile Durkheim’s concept of social pathology described breakdowns in norms and institutions as forms of collective illness. Michel Foucault’s work on biopolitics examined how power operates through institutions that regulate life, health, and behavior. Public health and development literature has frequently characterized corruption as a contagion that weakens governance and social trust. Systems theory has emphasized feedback loops, resilience, and tipping points in complex social systems.
These traditions employ medical or biological metaphors to describe social dysfunction. However, they do not integrate them into a unified, stage-based diagnostic model applied systematically across multiple institutions.
The present framework represents a synthesis of these intellectual lineages into a new analytical structure: a clinical progression model of societal disease that tracks corruption from predisposing vulnerabilities through latent pathology, acute outbreak, diagnosis, immune response, therapeutic struggle, and either remission or collapse. Its originality lies not in the metaphor itself, but in its formalization as a diagnostic system capable of comparative and longitudinal analysis.
This model is proposed as a hypothesis-generating framework rather than a proven theory. Like any medical model, it must be subjected to empirical testing across historical and contemporary case studies to determine whether its stages reliably appear, whether institutions interact in predictable ways, and whether early preclinical indicators can be identified before visible crisis emerges.
Core Stages of Societal Disease
Societal corruption is modeled as a progressive condition affecting interconnected institutions. Think of it as attacking a Nation’s foundational domains: family, education, economy, finance, healthcare, religion, government, law, elections, media, security, science, civil society, culture, and global systems.
Summary Table
| Stage | Clinical State | Institutional Reality |
| 1. Vulnerabilities | Predisposing Weakness | Misaligned incentives; power concentration; “fertile ground.” |
| 2. Latent Pathology | Subclinical Infection | Ethical decay is normalized; outward stability masks internal rot. |
| 3. Acute Outbreak | Visible Crisis | Corruption becomes overt; markets turn predatory; law is bent. |
| 4. Diagnosis | Rising Awareness | Public recognition of failure; whistleblowers identify patterns. |
| 5. Immune Response | Mobilized Resistance | Reform movements and ethical professionals push back. |
| 6. Therapeutic Struggle | Institutional Conflict | “Civil war” within sectors; fight between reform and entrenchment. |
| 7, Option A. Remission/Reform/Renewal | Structural Healing | Redesign of safeguards; restoration of transparency and trust. |
| 7, Option B. Destruction | Collapse | The society cannot withstand the illness and dies due to the extensive decay it has suffered. |
Detail
Stage 1: Vulnerabilities (Predisposing Weaknesses)
No illness begins with symptoms; it begins with weakened defenses. Societies likewise develop structural vulnerabilities such as misaligned incentives, opacity, concentration of power, and erosion of ethical norms that create conditions in which corruption can emerge.
In families, economic pressures may prioritize loyalty over law; in education, credentials over truth; in markets, profit over fairness; in finance, complexity over accountability. Healthcare may drift toward bureaucracy, religion toward hierarchy, and government toward unchecked discretion. These conditions are not corruption themselves but constitute fertile ground for it, often dismissed as routine inefficiencies.
Stage 2: Latent Pathology (Subclinical Infection)
Vulnerabilities allow corruption to embed quietly. Institutions appear functional, yet subtle distortions take root: conformity replaces inquiry, insider advantage replaces merit, and ethical compromise becomes normalized through rationalization.
This stage is particularly dangerous because outward stability masks internal decay. Norms shift gradually, and expectations recalibrate to accommodate misconduct without recognizing it as abnormal.
Stage 3: Acute Outbreak (Visible Crisis)
External shocks such as economic collapse, war, or leadership vacuums activate latent pathology. Corruption becomes overt: nepotism dominates organizational life, curricula become politicized, markets turn predatory, courts bend to power, elections lose legitimacy, and media fragments into propaganda ecosystems.
Feedback loops accelerate decline as distrust fuels manipulation and institutional failures reinforce one another. Symptoms become socially visible as injustice, dysfunction, and widespread loss of confidence.
Stage 4: Diagnosis (Rising Awareness)
Crisis forces recognition. Citizens, professionals, and watchdogs begin identifying patterns of favoritism, suppression of truth, and elite capture. Families debate loyalty versus integrity; educators expose distortions; journalists map networks of influence; communities demand accountability.
Denial persists among beneficiaries of corruption, but awareness spreads, creating the precondition for collective response.
Stage 5: Immune Response (Mobilized Resistance)
Diagnosis activates social defense mechanisms: whistleblowers, reform movements, investigative journalism, ethical professionals, and civic organizations. Institutions attempt to restore function through transparency, rule enforcement, and norm renewal.
This phase remains fragile. Corruption adapts through disinformation, intimidation, and legal obstruction. Nonetheless, the shift from passive acceptance to active resistance marks a decisive turning point.
Stage 6: Therapeutic Struggle (Institutional Conflict)
Defensive forces confront entrenched corruption directly. Institutions face existential choices: reform leadership or entrench it; redesign incentives or preserve opacity; empower oversight or tolerate impunity.
Outcomes diverge across sectors. Some achieve containment, while others deteriorate further. The society as a whole approaches a threshold between recovery and systemic failure.
Stage 7, Option 1: Remission, Reform, Renewal (Structural Healing)
Where resistance succeeds, corruption recedes into remission. Institutions rebuild through redesigned safeguards such as transparency mechanisms, ethical training, distributed authority, and accountability systems. Families emphasize responsibility, science demands replication and integrity, and global bodies enforce shared standards. These reforms must withstand future stress tests, as durable recovery requires resilience against renewed shocks. Renewal occurs when institutions mutually reinforce integrity: ethical families, truth-oriented education, fair markets, impartial law, and independent media. Corruption becomes manageable, analogous to a chronic but contained condition.
Stage 7, Option 2: Destruction (Structural Collapse/Systemic Inversion)
Where the immune response fails or is co-opted, the pathology achieves systemic inversion, a terminal state where the institution’s original purpose is actively weaponized against its intended goal. The social organism loses its functional coherence and moral legitimacy as predatory networks of insiders liquidate long-term institutional health for short-term private gain. In this stage, trust is entirely depleted, leaving behind “Zombie Institutions” that appear functional on the surface but exist solely for self-entrenchment and the extraction of remaining resources from the public.
The legal system in this state ceases to be a shield for the citizen and becomes a cudgel for the powerful, applied selectively to punish dissenters while granting absolute immunity to pathogenic networks. This represents a total hijacking of the society’s defensive systems, leading to a state of epistemic closure where truth is no longer a value to be discovered but a decree to be obeyed. Education and media transform into engines of total compliance, and science is reduced to a state-sanctioned liturgy. Collapse is rarely a singular event but rather the final loss of the society’s ability to self-correct, resulting in a fragile structure that dissolves into fragmentation or total absorption by more coherent external systems.
Theoretical Example: Scientific Pathology
Stage 1: Vulnerabilities (The “Rigged” Market)
The disease begins when the system stops rewarding accuracy and starts rewarding headlines. When funding is concentrated in a few hands, scientists become “courtiers” trying to please the king rather than “explorers” trying to find the truth.
- Markers: Grant power held by a few bureaucrats; “Publish or Perish” metrics; the death of tenure.
Stage 2: Latent Pathology (The “Accounting Fraud”)
This is where the “Silent Infection” of the Replication Crisis happens. Scientists start “cooking the books”—manipulating data (p-hacking) to get a result that looks successful so they can get their next “paycheck” (grant).
- Markers: “Pal-review” (friends approving friends); burying negative results; subtle exclusion of dissenters.
Stage 3: Acute Outbreak (The “Propaganda” Fever)
During a crisis, the system breaks. Science is no longer a tool for inquiry; it is a rhetorical cudgel. “The Science” is used to justify power, and the institution begins to act like a PR firm for the state.
- Markers: Censorship of peer-reviewed dissent; retraction of “inconvenient” studies; scientists as partisan activists.
Stage 4: Diagnosis (The Public Audit)
The public notices that the “experts” are consistently wrong or biased. Independent “data detectives” and citizens begin to audit the work, finding faked images and fraudulent spreadsheets that the official journals ignored.
- Markers: Viral exposure of fraud; loss of trust in scientific authority; rise of independent meta-science platforms.
Stage 5: Immune Response (The Reform Movement)
The “antibodies” of science—skepticism and transparency—activate. Reformers demand Open Science, insisting that the “black box” of the lab be opened for public inspection.
- Markers: Whistleblowers; “Pre-registered” report requirements; alternative peer-review systems.
Stage 6: Therapeutic Struggle (The Institutional Conflict)
The “Gatekeepers” (who run the broken system) fight the “Reformers” (who want to fix it). It is a battle between those who want to protect the institution’s reputation and those who want to protect the scientific method.
- Markers: De-platforming of reformers; legal battles over data; creation of “Parallel Institutions.”
Stage 7: Renewal vs. Collapse
Collapse: Science becomes a State Religion where data is subordinate to power.
Renewal: Science returns to a Self-Correcting Market where truth is the highest value.
The Overall Model: Limitations and Areas for Development/Theoretical Refinement
While the proposed medical model offers a structured diagnostic lens for analyzing societal corruption, several conceptual dimensions warrant further development to enhance its analytical precision and empirical usefulness.
1. No Remediation Model Provided
A final critical limitation of this framework is the distinction between diagnosis and remediation. While this model identifies the stages and symptoms of societal disease, it does not prescribe a comprehensive “cure” or a manual for institutional repair. Identifying the pathology of a system is a distinct analytical task from designing the interventions required to heal it. Any future “therapeutic model” aimed at fixing these institutions may not directly correspond to the stages of corruption outlined here; for instance, the steps to reverse systemic collapse may require entirely different mechanisms than those used to prevent initial vulnerability. Therefore, this framework should be viewed as a diagnostic map rather than a treatment plan, serving as the necessary first step of clinical recognition before a separate, restorative strategy can be developed.
2. Corruption Is Sometimes A Secondary Pathogen
The framework currently treats corruption as the primary societal pathogen. However, medical analogies suggest the importance of distinguishing between different types of disease mechanisms. In particular, a refined model could differentiate between external infections and internal autoimmune responses.
External infections may include foreign interference, transnational criminal networks, resource shocks, or technological disruptions that destabilize institutions from outside the system. Internal autoimmune responses occur when a society’s own defensive mechanisms—such as legal systems, security institutions, or regulatory bodies—become overactive or distorted and begin harming the social body they were designed to protect. Examples include excessive surveillance, politicized prosecutions, or regulatory overreach that erodes trust and legitimacy.
This distinction would allow the model to account for cases in which institutional breakdown is not driven primarily by predatory actors but by defensive systems that misfire and generate systemic damage. Incorporating this dimension would move the framework closer to clinical medicine, where identifying disease etiology is essential for appropriate treatment.
3. Comorbidity and the Multiplier Effect
Medical conditions rarely occur in isolation, and social pathologies are no different. A critical refinement of this model involves incorporating the concepts of comorbidity and syndemics, where multiple institutional failures cluster and interact to produce compounded systemic harm.
- Comorbidity: Rather than viewing corruption as a series of isolated incidents, a networked perspective recognizes that the “viral load” of one failing institution inevitably overflows into others.This creates a multiplier effect where the total degradation of the social organism is far greater than the sum of its individual parts. For instance, a pathology in the financial sector does not merely stay there; it generates downstream effects that weaken the family through economic precarity, degrade education through underfunding, and compromise the media through its dependence on concentrated capital.
- The Multiplier Effect: As one institution enters a state of Acute Outbreak, it functions as a primary driver of contagion for those still in the Latent or Vulnerable stages. Dysfunction in the media, for example, acts as an accelerant that intensifies political polarization, which in turn weakens legal accountability and distorts scientific authority. When the “immune systems” of multiple sectors fail simultaneously, the feedback loops of corruption become self-sustaining and increasingly difficult to interrupt. Recognizing these interdependencies allows the model to identify which institutions serve as “super-spreaders” of institutional decay and which act as vital buffers that might prevent a localized infection from becoming a systemic collapse.
By adopting this networked understanding, the framework moves beyond a simple linear progression toward a more sophisticated map of institutional disease. This perspective is essential for identifying strategic leverage points where interventions can be most effective. Rather than treating each institution in isolation—an approach that often fails due to the cross-contamination of neighboring sectors—reformers can aim to disrupt the specific feedback loops that allow comorbidity to thrive. Ultimately, a society’s health is determined not just by the integrity of its individual parts, but by the strength of the connective tissue that prevents the failure of one system from triggering a cascading, irreversible decline across the entire social body.
4. Who Is The Doctor?
If society is conceptualized as the patient, a central unresolved question concerns the identity and legitimacy of the physician. In political and social contexts, this role is deeply contested. Potential candidates include intellectual elites, judicial systems, professional experts, civic movements, or the general public acting through democratic mechanisms.
Each option carries risks. Concentrating diagnostic and therapeutic authority in elites may produce technocratic overreach. Judicial or regulatory dominance risks politicization. Popular movements risk emotionalism or factional capture. These dangers parallel the medical concept of iatrogenesis, in which treatment itself causes harm.
Addressing this “physician problem” is essential for preventing the model from becoming a justification for coercive or paternalistic interventions. A more robust formulation would emphasize plural and distributed diagnostic authority, transparency of evidence, and continual feedback between institutions and citizens. In this sense, societal healing may require not a single physician but a network of overlapping and self-correcting evaluators.
Incorporating the risk of healer-induced harm strengthens the model’s neutrality and underscores that even well-intentioned reforms can deepen pathology if poorly designed or insufficiently constrained.
Further Reading and Related Resources (Annotated)
Each resource listed below represents a foundational pillar in its respective field—philosophy, sociology, political theory, economics, systems theory, or public health. Together, they provide the conceptual “nutrients” that inform the present diagnostic framework without duplicating it.
Plato, The Republic
Field: Philosophy / Political Philosophy
Introduces the earliest articulation of the body politic, treating society as a natural organism whose health depends on harmony among its parts. Establishes the foundational metaphor that social disorder can be understood as a form of disease.
Thomas Hobbes, Leviathan
Field: Political Philosophy
Conceptualizes the state as an artificial body created to prevent collapse. Hobbes explicitly identifies sedition and faction as “distempers” of the commonwealth, aligning closely with the Acute Outbreak stage of this model.
Émile Durkheim, The Division of Labor in Society
Field: Sociology
Develops the concept of social pathology and argues that while some deviance is normal, excessive deviance becomes pathological. Provides a threshold-based logic for diagnosing institutional dysfunction.
Michel Foucault, Discipline and Punish
Field: Philosophy / Social Theory
Analyzes how power operates through institutions that regulate bodies and populations. His concept of biopower informs the distinction between healthy immune responses and autoimmune disorders within social systems.
Hannah Arendt, The Origins of Totalitarianism
Field: Political Theory / History
Explores how propaganda, bureaucracy, and institutional decay generate systemic political pathology. Illustrates transitions from latent pathology to acute outbreak and collapse.
James C. Scott, Seeing Like a State
Field: Political Science / Anthropology
Shows how technocratic “cures” imposed from above often fail by ignoring local knowledge. Directly informs the Physician Problem and the risk of iatrogenic harm.
Karl Polanyi, The Great Transformation
Field: Economic History / Political Economy
Explains how disembedding markets from society destabilizes social institutions. Provides the etiology of institutional disease by identifying economic disruption as a causal mechanism.
Douglass North, Institutions, Institutional Change and Economic Performance
Field: Economics / Institutional Theory
Analyzes how formal and informal rules shape incentives and behavior. Provides the anatomy of institutional disease by explaining structural vulnerabilities.
Donella Meadows, Thinking in Systems
Field: Systems Theory / Environmental Science
Supplies the logic of feedback loops, leverage points, and resilience. Functions as the physiology of the framework, explaining immune response and reform.
Robert Putnam, Bowling Alone
Field: Sociology / Political Science
Documents the erosion of social capital and civic trust. Supports the Vulnerability stage by showing how weakened communal bonds create susceptibility.
Transparency International, Global Corruption Report
Field: Political Science / Public Policy
Provides empirical data on corruption across institutions worldwide. Supplies indicators for testing the diagnostic stages of the model.
World Health Organization, Corruption and Health
Field: Public Health / Global Governance
Demonstrates how corruption directly damages healthcare systems and population outcomes, bridging medical and institutional analysis.
Jared Diamond, Collapse: How Societies Choose to Fail or Succeed
Field: Geography / History / Environmental Studies
Offers comparative historical cases of collapse and resilience. Supports the model’s two end states of renewal versus collapse.
Albert O. Hirschman, Exit, Voice, and Loyalty
Field: Economics / Political Theory
Explains how individuals respond to institutional decline through withdrawal, protest, or allegiance. Informs the Diagnosis and Immune Response stages.
Notes
- This framework is a work of sociological analysis and institutional theory; it is not a clinical medical document. The author is a sociologist, not a medical doctor. While this model utilizes medical metaphors—such as “pathology,” “immune response,” and “remission”—these are conceptual tools designed to identify and analyze patterns of systemic corruption.
- This framework is proposed as a hypothesis-generating model for empirical testing across the social sciences. With some development, it could eventually provide a diagnostic lens for social intervention and institutional design. However, it is not meant as a literal tool for medical diagnosis or policy intervention at this time.
- AI was used to research, write, and fact-check this essay. The original sociological hypotheses are the author’s own.

You must be logged in to post a comment.